
Tooth shaping with composite after anterior tooth transplantation
Patient history
After falling at a swimming pool in 2000 and avulsion of the two central incisors 11 and 21 (both teeth were lost during the fall), the patient underwent transplantation of teeth 34 and 44 into region 11 and 21. Seven years later, the patient presented for consultation about the further treatment of the transplanted premolars. Prior to the consultation, the patient had been satisfied with the treatment to date. The patient was simultaneously undergoing orthodontic treatment with regular radiographic follow-up of the region 11/21. The apical region of the transplanted premolars was unremarkable with no signs of root resorption.


Treatment planning
After evaluation of the clinical and radiographic findings, it was planned to reshape the transplanted premolars 34 and 44 into central incisors through a minimally invasive procedure. The patient refused other treatment alternatives such as the fabrication of all-ceramic veneers and surgical crown lengthening (vestibular extension) for harmonizing the gingival course due to the highly invasive nature of the procedures.

Treatment course
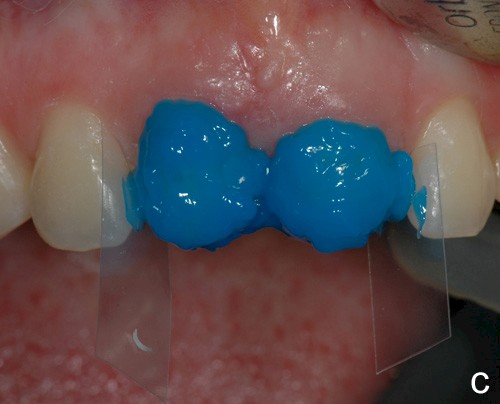
A wax-up was fabricated (Fig. 2) for informing the patient about various treatment options and to evaluate the anticipated amount of substance that would be lost as the result of the preparation measures.
Based on the silicone key fabricated on the wax-up, an intraoral mock-up was fabricated with a provisional plastic material to visualize the targeted treatment results. Due to the thickness of the wax-up and the position of the transplanted premolars in the dental arch, it was agreed with the patient, who was very satisfied with the mock-up, to shape the restoration more delicately in a vestibular direction.


The teeth were then cleaned with a fluoride-free prophylaxis paste. The shade was then selected. The material ESTELITE SIGMA QUICK (Tokuyama Dental) was used as a composite system. In this system, an extra-opaque dentin mass is available with the shade OPA2, which was used to build up dentinal core of the incisors that is not supported by the dental hard tissues. The following shades were used: OPA2, OA2, OA3 (dentin masses), A2, A3 (enamel masses), CE (Clear Enamel, special-effect mass for translucent effects), OPA2 (flowable). A diamond finisher was used minimally invasively to roughen the enamel surface of the transplanted premolars, which was then conditioned for 30 seconds with 37% orthophosphoric acid (Conditioner 36, Dentsply, Konstanz, Germany) and pretreated with adhesive (Heliobond, Ivoclar Vivadent, Ellwangen, Germany). The silicone key was then used to build up the posterior wall with a thin layer of the flowable of shade OPA2. The various dentin masses were then modeled in several layers: OPA2 as the opaque core, OA3 cervically and OA2 toward the incisors. An approx. 1 mm-wide area in the region of the incisal edge was left open that was filled with a thin layer of special-effect mass (CE). To achieve the "halo effect", a very thin layer of OA2 was modeled directly at the incisal edge. The dentinal core was then overcoated with the enamel masses (A2 incisal, A3 cervical).
After the final polishing, the teeth were fluoridated (Biflourid, VOCO, Cuxhaven, Germany).












The following images show the restorations at follow-up appointments after 4 weeks, 4.5 months and 14 months.






After completion of the treatment, the patient agreed to present for follow-up sessions at 6-month intervals.
Summary and discussion
The case study presented here depicts the reshaping of two premolars after autogenous tooth transplantation after anterior tooth trauma in which the two central incisors were avulsed and were no longer available for replantation due to loss.
Several case reports have been published on the reshaping of transplanted premolars to replace anterior teeth in which both composite restorations and all-ceramic veneers were fabricated as measures for reshaping.
In this case, at the patient's request, information was provided about a variety of approaches and a minimally invasive procedure was used to fabricate composite restorations. A wax-up was fabricated and a silicone key was used to build up the posterior wall from a very thin layer of flowable. Since the occlusal contacts are located in the area of the hard tooth structure, this approach proved to be feasible.
The patient is satisfied with the treatment results achieved. During the 14-month observation period there were no signs of restoration failure.

Author:
Professor Dr Anne-Katrin Lührs
Senior Physician at the Department of Conservative Dentistry, Periodontology and Preventive Dentistry, Hannover Medical School (Director: Professor Dr W. Geurtsen)
Carl-Neuberg-Str. 1
DE-30625 Hannover
Germany
Phone: +49 511 5324815
https://www.mhh.de/kliniken-der-mhh/klinik-fuer-zahnerhaltung-parodontologie-und-praeventivzahnmedizin