

OMNICHROMA FLOW: The perfect complement to the pasty original
The fact that product innovations have a market significance is often shown by the fact that "market competitors" take up the same topic and bring products with the same application focus, sometimes even improved in detail or adapted to further indications. In the field of restoratives, one can mention, for example, bulk-flow composites and universal adhesives. In the meantime, they are available in all variations from almost all manufacturers. There is a similar situation with the "revolution" of bringing a single composite colour for all shades of teeth, as TOKUYAMA DENTAL managed to do three years ago with OMNICHROMA. The addition of a flow variant to this product idea is absolutely welcome and rounds off the application possibilities excellently.
The trend towards simplification of composite shade ranges has been immanent in recent years: sets with more than 30 shades for the perfect individual shade combination may be justified in individual cases [6, 32-34]; in broad application, however, they tend to discourage. Enamel Plus HRi (Micerium) already got by with a significantly reduced range of materials - Vanini and Hugo, among others, have already shown what can be conjured up from it [4, 21, 22, 34]. Amaris (VOCO) [7], Ceram.X mono & duo (Dentsply Sirona) [8, 9] Ceram.X Spectra ST (Dentsply Sirona) [11] Filtek Universal (3M) [12, 13] or Clearfil Majesty ES-2 (Kuraray) continued the trend towards simplification.
Already in 2019, TOKUYAMA DENTAL came up with a widely acclaimed novel composite that covered only one restoration shade (supported by a "blocker") for all shade indication ranges [10]. Particularly with regard to differentiation in shade selection, difficulties often arise in matching details when there is too large a selection of restoration shades: Is it now an A2 or a D2 - or a little more grey dominance? It is nice to see that the chameleon effect of materials such as OMNICHROMA, which is now really apparent for the first time, actually makes things easier: Less time spent on shade selection combined with coherent aesthetic results. Thus, the success story [1-3, 5, 8, 14-17, 20, 23-29, 31] of direct aesthetic and adhesive anterior restorations continues consistently under the aspect of user facilitation and reduced necessary stock-keeping.
The aforementioned shade selection is particularly difficult with cervical defects [18, 19], as they often extend the defects far into the labial surface [17]. Here, the cavity passes through a wide variety of shade values - from a Vita A3.5 in the tooth neck area to a Vita A2 shade in the centre of the labial surface. Of course, this can be adequately restored aesthetically with an adapted layering concept, but this is often disproportionately expensive for a Class V restoration.
This is why a material such as OMNICHROMA scores very well in indication areas of the cervical region, since in principle one does not have to worry about the shade selection at all. Only the addition of the OMNICHROMA BLOCKER prevents undesired shining through of shade-mismatched backgrounds.
The two case studies presented below show the application of OMNICHROMA in different cervical defects in combination with OMNICHROMA FLOW and the OMNICHROMA BLOCKER FLOW: sometimes OMNICHROMA FLOW alone, sometimes in combination with OMNICHROMA BLOCKER FLOW, sometimes as a triple combination of OMNICHROMA FLOW, OMNICHROMA BLOCKER FLOW and the pasty OMNICHROMA.
Case 1
Multiple cervical defects
The 41-year-old patient had multiple cervical lesions caused by incorrect brushing technique as well as parafunctions (Fig. 1). After changing the tooth brushing technique and consistently wearing a nightly bite splint in the lower jaw, it was now time to treat the cervical defects on teeth 12 and 13 that bothered her the most. The bonding surfaces of both teeth were touched up with a fine-grain micro-preparation diamond (8830M, Komet, Lemgo) and the discolouration lying in the cavity was also removed in the same operation. No further preparation was carried out. As the sulcus was healthy and firm, a thread insertion, which is often the most sensible way of controlling contamination in tooth neck defects [17], was dispensed with in favour of individual shuttering using a Frasaco strip (Frasaco, Tettnang). This veneering technique (Fig. 2) has the advantage of automatically ensuring a perfect cervical finish of the restoration under ideal conditions of contamination control with a correctly seated strip fixed with small wooden wedges (KerrHawe, Bioggio, Switzerland) (Fig. 3). The filling material can later fill the acute angles perfectly - provided it has the right consistency to flow or adapt here without defects.
The entire cavity was conditioned with 37.5% low-viscosity phosphoric acid gel (Gel Etchant, Kerr, Orange, CA, USA, Fig. 3). The transparent Frasaco strip allows perfect visual control of the correct application of etching gel to filling material, as it can always be viewed from the labial side. Figure 4 shows the clinical situation after rinsing off the etching gel. A traditional multi-bottle system was used as the adhesive (Optibond FL, Kerr).





In the present case, a low-viscosity restorative material was required in any case because the acute angles between the cervical cavity margin and the Frasaco strip could be reached, so this could also be used as the restorative material of choice for the entire cavity because of the small defect size. The prerequisite is a suitable stability of the material so that the filling material can be "painted on" with the cannula without flowing away.
The shade selection resulted in a Vita shade A1 for tooth 12 and Vita shade A2 for tooth 13. With conventional materials, it would now have been necessary to provide two different shades of restorative materials. OMNICHROMA FLOW (TOKUYAMA DENTAL, Tokyo, Japan) was chosen both because of the required consistency and because of the automatic shade adaptation, as both cavities could then be restored with the same filling material. As tooth 12 showed a distinct discolouration of the dentin in the cervical area, the new OMNICHROMA BLOCKER FLOW was applied selectively to ensure optical masking of this discoloured area. OnlyOMNICHROMA FLOW without the blocker was used on tooth 13. Figure 5 shows the final result of the OMNICHROMA FLOW restoration after finishing and polishing. The result shows that such defects can be created margin-tight, in correct anatomical shape and in perfect shade matching even with the low-viscosity OMNICHROMA FLOW alone, without being covered by the pasty version. The patient was very satisfied with the final result; however, she did not wish to have tooth 21 restored. Both restorations were charged as partly private fillings with a co-payment of €60 each.
Case 2
Restoration of a solitary tooth neck defect
A similar case shows the restoration of tooth 12 of a 50-year-old patient: The patient, who is now functionally stable, is disturbed by the cervical defect on tooth 12 (Fig. 6). The Unica anterior matrix (Polydentia, Mezzovico-Vira, Switzerland), adapted proximally and sealed with 2 Composi-Tight 3D Fusion Wedges (Garrison Dental Solutions, Spring Lake, Mi, USA, fig. 7), was used to form the veneer and thus isolate the defect. The adhesive pretreatment was carried out in the same way as in the previous case (Fig. 8).
Here, too, the challenge is to fill the difficult-to-reach acute angles between the cavity and the Unica matrix with composite material without bubbles. In contrast to the first case, the metal Unica matrix does not allow visual control of the filling material adaptation from labial. In this case, you either have to trust that the material is adapted correctly or you proceed according to the "snowplough technique": This procedure allows the flowable to be pressed into the acute angles by the pressure of a subsequently applied pasty composite material (without separate polymerisation of the flowable) and thus prevents undercuts as well as air bubble inclusions. The prerequisite, however, is a tight fit of the matrix! This technique was first described by Opdam et al. in 2003 for Class I cavities [30]; it was later taken up by the Heidelberg conservative dentistry for the anterior region and also established there [35]. Thus, this treatment indication was predestined for the combination of OMNICHROMA and OMNICHROMA FLOW, which were polymerised simultaneously.


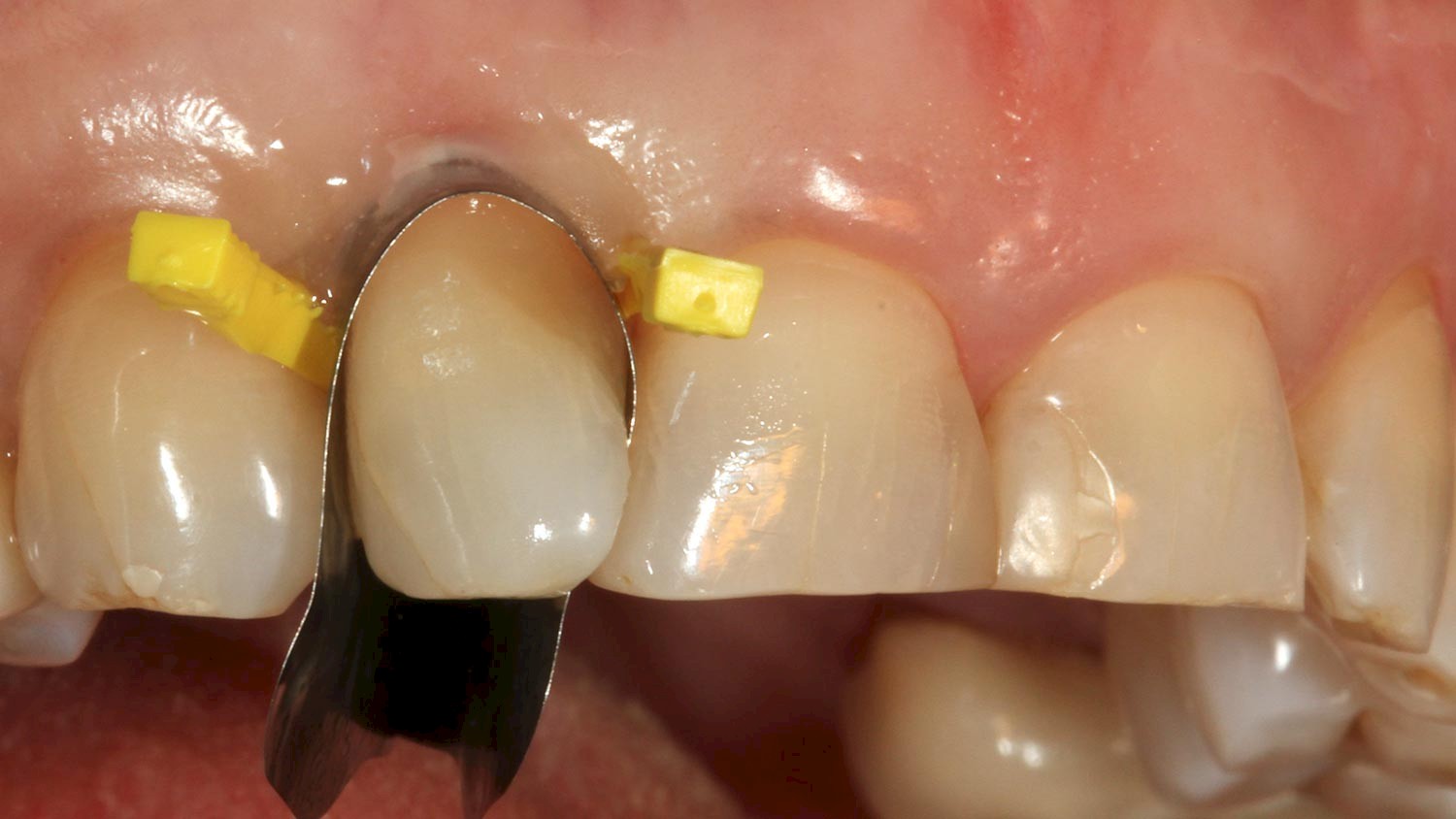


Figure 9 shows the treatment situation immediately after finishing and polishing, and figure 10 shows a further check after six months. Thanks to the automatic shade adaptation of both OMNICHROMA and OMNICHROMA FLOW, a perfect shade match was achieved here as well. The gloss level of the extremely fine-grained filling material was also completely retained. The patient was amazed at the current possibilities of an aesthetic and minimally invasive defect restoration. The fact that this shade match was primarily due to the simplicity of the selected restorative material did not need to be explained to the patient in more detail....
Conclusion
A simple and structured approach to cervical restorations does not in any way mean having to compromise on the achievable functional and aesthetic treatment outcome. The choice of restorative material in the two cases presented was limited to the most suitable consistency in each case and the question of the need for a blocker to be used. The shuttering of the presented defects required a considerably higher deviation and implementation effort than the restoration itself.

Author:
Prof. Dr Claus-Peter Ernst
Professor, Polyclinic for dental conservation, University Medicine of the Johannes Gutenberg-University Mainz
Dental clinic medi+
Haifa-Allee 20
DE-55128 Mainz
Germany
Phone: +49 6131 4908080
ernst@mediplusmainz.de
https://mediplusmainz.de
- Allgeier S, Hahn B, Krastl G. Direkte Frontzahnrestaurationen aus Komposit. Wissen Kompakt 2019; 13 (3): 1903-112.
- Araujo E, Perdigao J. Anterior Veneer Restorations – An Evidence-based Minimal-Intervention Perspective. J Adhes Dent 2021; 23: 91-110.
- Báez Rosales A, De Nordenflycht Carvacho D, Schlieper Cacciutolo R, Gajardo Guineo M, Gandarillas Fuentes C. Conservative Approach for the Esthetic Management of Multiple Interdental Spaces: A Systematic Approach. J Esthet Restor Dent. 2015, 27: 344-354.
- D'Arcangelo, C, Vanini, L & Rondoni, Gd & Pirani, M, Gattone, M. Wear Properties of a Novel Resin Composite Compared to Human Enamel and Other Restorative Materials. Oper Dent 2014; 39. 10.2341/13-108-L.
- Demarco FF, Collares K, Coelho-de-Souza FH, Correa MB, Cenci MS, Moraes RR, Opdam NJ. Anterior composite restorations: A systematic review on long-term survival and reasons for failure. Dent Mater 2015; 31: 1214-1224.
- Devoto W, Saracinelli M., Manauta J. Composite in everyday practice: how to choose the right material and simplify application techniques in the anterior teeth. Eur J Esthet Dent 2010; 5: 102.
- Ernst CP. Der neue Trend zum Minimalismus. Einfache Schichtung ästhetischer Frontzahnrestaurationen – trotz oder wegen reduzierter Farbpalette? ZMK 2008; 24: 330-339
- Ernst CP. Direkte Frontzahnrestaurationen aus Komposit - aktuelle Studienlage und Fallbeispiele. ZMK 2017; 33; 2-8.
- Ernst CP. Schichtkonzepte bei vereinfachten Frontzahnkomposit-Systemen. ZMK 2018; 34: 570-591.
- Ernst CP. Ein einziges Komposit – eine Farbe für alles? ZMK 2019; 35: 783-785.
- Ernst CP. Ein praxistaugliches neues Schichtkonzept für Ceram.x Spectra ST ZMK 2020; 36: 48-59.
- Ernst CP. Diastemaschluss mit einer einzigen Universalfarbe. ZMK 2020; 36: 220-225.
- Ernst CP. Zervikale Approximalanbauten. ZMK 2020; 36: 368-375.
- Ernst CP. Haltbarkeit von direkten Kompositaufbauten an Schneidezähnen nach FZT-Versorgung. ZMK 2021; 37: 90-102.
- Ernst CP. Fallbeispiele zum ästhetischen Indikationsspektrum von Tetric Prime im Frontzahnbereich. ZMK 2021; 37 (9): 542-552.
- Frese C, Schiller P, Staehle HJ. Wolff D. Recontouring teeth and closing diastemas with direct composite buildups: a 5-year follow-up. J Dent 2013; 41: 979-985.
- Hahn B, Soliman S, Allgeier S, Krastl G. Direkte ästhetische Restaurationen im Frontzahngebiet. Der Freie Zahnarzt 2021; 65 (12): 60-678.
- Hajto J. Freud und Leid mit direktem Komposit. Teil 1: Adhäsive, Indikationsstellung und Chamäleoneffekt . Teamwork 2006; 9: 50-63.
- Hajto J. Freud und Leid mit direktem Komposit. Teil 2: Schichttechnik, Versorgung multipler Füllungen im Frontzahnbereich. Teamwork 2006; 9: 86-97.
- Heintze SD, Rousson V, Hickel R. Clinical effectiveness of direct anterior restorations--a meta-analysis. Dent Mater 2015; 31: 481-495.
- Hugo B. Optimale Approximalkontakte – Neue approximale Matrizen- und Aufbautechnik bei Frontzahnfüllungen. Ästhetische Zahnmedizin 2001; 3: 241-250.
- Hugo B. Ästhetik mit Komposit. Quintessenz Verlags GmbH, Berlin, 2008 ISBN 978-3938947-55-59.
- Klaff MP, Ward GT. Composite technic for restoration of malformed teeth. Dent Surv 1973; 49: 34-36.
- Klaiber B. Alles noninvasiv - Zahnformveränderung, Lückenschluss, Reduktion schwarzer Dreiecke. zm 2006; 96: 52-59.
- Krastl G, Weiger R. Frontzahnrestaurationen: Brauchen wir überhaupt Keramik? Die Quintessenz 2010; 61. 511-520.
- Krastl G. Composite – das Mittel der Wahl. ZWP 2011; 11: 74-78.
- Lenhard M. Ästhetische Frontzahnrestaurationen mit Komposit. Quintessenz 2004; 55: 961-976.
- Lenhard M. Diastemaschluss mit Kompositrestaurationen. Eur J Esthet Dent 2008; 3: 282-292.
- Lührs AK. Diastemaschluss mittels direkter Technik im Frontzahnbereich. Deutsch Zahnärtzl Z 2011; 66, 628-635., Krastl G. Composite – das Mittel der Wahl. ZWP 2011; 11: 74-78.
- Opdam NJ, Roeters JJ, de Boer T, Pesschier D, Bronkhorst E. Voids and porosities in class I micropreparations filled with various resin composites. Oper Dent 2003 ; 28: 9-14.
- Romero MF. Esthetic anterior composite resin restorations using a single shade: Step-by-step technique. J Prosthet Dent 2015; 114: 9-12.
- Vichi A. et al. Influence of thickness on color in multi-layering technique. Dent. Mater. 2007; 23 (12): 1584-1589.
- Villarroel M, Fahl N, De Sousa AM, De Oliveira OB Jr. Direct esthetic restorations based on translucency and opacity of composite resins. J Esthet Restor Dent. 2011; 23(2):73-87.
- Vanini L, Mangani F, Klimovskaia O. Conservative Restoration of Anterior Teeth. ACME-Verlag 2007; 2. Auflage.